
Google Ads
Google Ads
Google Ads
An Unprecedented Complication, never seen ,never heard in My 17-Year Career in Anesthesia
An Unprecedented Complication, never seen ,never heard in My 17-Year Career in Anesthesia

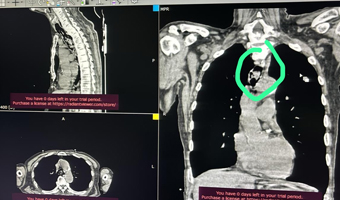
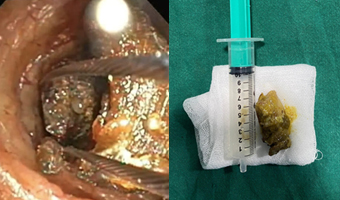
Recently, a routine adenotonsillectomy turned into a life-threatening challenge for a 10-year-old girl, highlighting the unpredictable nature of medical procedures. The patient, an ASA I with no underlying health conditions, underwent a smooth nasotracheal intubation using a 5.5 ID PVC endotracheal tube (ETT), with a Cormack-Lehane score of 1. However, during the procedure, the ENT surgeon discovered that the ETT had broken into two pieces, leaving the distal part likely lodged in the trachea.
The Hidden Dangers of Outdated Medical Practices: Insights from Dr. Udaya Bhaskar Tupakula
The Hidden Dangers of Outdated Medical Practices: Insights from Dr. Udaya Bhaskar Tupakula
We live in a world where technology has advanced immensely—rovers are on Mars, humans have walked on the Moon, and smartphones with 5G and AI are in our hands. Yet, when it comes to healthcare, outdated and primitive practices still harm our most valuable asset: the human body. For the past 14 years, I’ve worked to raise awareness about the importance of modern, evidence-based medical treatments.

But recently, the number of patients suffering from complications due to outdated methods has made this mission more urgent. In areas around Tirupati, like Puttur/Eslapuram and Kallur, we see many victims of these outdated treatments. The issue affects everyone, regardless of education or social status. Many people avoid surgery out of fear or cost concerns, while others trust ancient methods like Shalya medicine. What they don’t realize is that these practices often cause more harm than good. One of the biggest misconceptions is that all fractures should be treated the same way. I’ve seen patients with minor injuries treated with outdated methods like chicken wire or makeshift bandages. These methods are not just ineffective—they also undermine the expertise of modern orthopedic care. I’ve witnessed the consequences of this firsthand. Bones heal in misaligned ways, and patients suffer nerve and blood supply damage from improperly applied implants. By the time these patients seek treatment, it’s often too late for a simple fix. Some argue that surgery is too expensive, but free treatment is available at local hospitals or at Tirupati Ruya hospitals. The real cost is the long-term damage caused by avoiding proper care. Attempting to fix complications with outdated methods only makes things worse. In some cases, what could have been a minor procedure turns into a complex surgery with poor results.
As a doctor, it’s frustrating to see patients suffer from preventable complications. But my mission remains to educate people and help them avoid these outdated practices in the future.
Success in Retroperitoneal Tumor Surgery
Success in Retroperitoneal Tumor Surgery
Nagamani and Sai Nath, parents from Proddatur, brought their 7-month-old baby to Shanthiram Hospital, concerned about severe bloating, abdominal swelling, and vomiting. Scans revealed a large mass in the baby’s abdomen (Retroperitoneal Tumor). Further tests showed that the baby had critically low hemoglobin levels (6.0),

prompting a blood transfusion before surgery could be performed. During the surgery, the baby’s blood pressure dropped, and the mass was found to be wrapped around vital organs, resembling cancerous growth. The mass was sent for further evaluation ie, histopathology and IHC evaluation, this would give us further direction of management in this child, currently, the child is relieved from the symptoms, further, the team will involve appropriate specialists for further medical management in this child if needed, stated Dr Ravinder leading the team
However, under the expert guidance of Pediatric Surgeon Dr. Ravinder, along with the anesthesia team led by Dr. Ravi Teja and Dr. Chiranjeevi, the retroperitoneal tumour surgery was completed. The mass was carefully removed without damaging surrounding organs, which the experts like the pediatric surgeon and the baby was safely discharged back home. The parents expressed their heartfelt gratitude to Dr. Ravinder, the anesthesia team, and the hospital management for giving their child a second chance at life.
Laparoscopic Repair of Rare Left-Sided Primary Upper Lumbar Hernia by Dr. Satish Kumar Raju. S
Successful Laparoscopic Repair of a Rare Lumbar Hernia
A 31-year-old man successfully underwent laparoscopic Transabdominal Preperitoneal (TAPP) mesh repair for a rare left-sided primary upper lumbar hernia, known as Grynfeltt-Lesshaft hernia. This condition is extremely uncommon, with fewer than 300 cases reported worldwide.

The patient reported intermittent swelling in the left superior lumbar region over the past year, which became more noticeable during coughing and reduced spontaneously. DR.SATISH KUMAR RAJU.S, Consultant General & Laparoscopic Bariatric surgeon at SLG HOSPITALS, Bachupally, Hyderabad, who examined the patient, found a lump in the upper left lumbar area that became more prominent during coughing. Imaging tests confirmed it was a Grynfeltt-Lesshaft hernia. To treat this, Dr. Raju and his team performed a minimally invasive surgery called Transabdominal Preperitoneal (TAPP) mesh repair. They used a 15×15 cm synthetic mesh to strengthen the affected area. The procedure went smoothly without any complications. The patient recovered well and was discharged just 24 hours after the surgery. Follow-up checkups showed no recurrence of the hernia, indicating a successful outcome.

What Makes Lumbar Hernias Rare and Complex?
Lumbar hernias are among the rarest types of abdominal hernias, accounting for less than 2% of cases. Grynfeltt-Lesshaft hernias are an even rarer subtype. Due to their location and mild symptoms, they can be difficult to diagnose. However, laparoscopic TAPP mesh repair, as demonstrated in this case by Dr. Satish Kumar Raju. S, is a highly effective, minimally invasive treatment option for such conditions. Early diagnosis and timely surgical intervention are essential for achieving the best results in rare and complex hernias like this one.
Hernia Surgery on 23-Day-Old Infant: Dr. M. Saravana Balaji Leads Rare Procedure, Only Fourth Known Case Worldwide
Hernia Surgery on 23-Day-Old Infant: Dr. M. Saravana Balaji Leads Rare Procedure, Only Fourth Known Case Worldwide
Chennai, 6 September 2024: A 23-day-old premature baby, born at just 28 weeks, has successfully undergone a rare and complex surgery to treat Amyand’s hernia, a condition where a ruptured appendix is located in the groin. This marks only the fourth known case worldwide involving a preterm neonate.
The infant developed an obstructed right inguinoscrotal swelling on the 23rd day after birth, prompting an emergency surgery. The procedure involved three key components: inguinal exploration to assess the groin area, appendectomy to remove the ruptured appendix, and herniotomy to repair the hernia by removing the hernia sac and fixing the abdominal wall defect.

Despite the delicate nature of the surgery, it was successfully completed within an hour, and the baby is now recovering well and gaining weight steadily under specialized care. Dr. M. Saravana Balaji, Consultant Pediatric Surgeon, who led the surgery, commented, “While neonatal hernias are relatively common in preterm babies, Amyand’s hernia is exceptionally rare, affecting less than 0.07% of these infants. In this case, the perforated appendix made it even more critical, with a mortality rate of up to 30% if untreated. Our team’s swift and expert intervention was crucial to saving this baby’s life.”
The surgical team also included Dr. Prathiba N, along with anesthesia experts Dr. K. Anand and Dr. Dheepak Kumaran, supported by NICU doctors Dr. S. Subash and Dr. Ashok C. Postoperatively, the infant received specialized care in the NICU to ensure proper recovery.
SRM Global Hospitals, where the surgery took place, has been recognized for its ability to manage complex and rare medical cases, setting a new benchmark in neonatal care.
Treating UTI In Children: When Does A Child Need To See A Pediatric Urologist?
Treating UTI In Children: When Does A Child Need To See A Pediatric Urologist?
Dr. Prabhu Karunakaran, consultant pediatric urologist at the Asian Institute of Nephrology and Urology, Hyderabad, emphasizes the importance of understanding urinary tract infections (UTIs) in both adults and children, as there are differences in risk factors and prevalence. In children, repeated UTIs require evaluation by a pediatric urologist since approximately 30 percent may have anatomical abnormalities, such as vesicoureteric reflux (VUR). UTIs are more prevalent in male infants, particularly those who are uncircumcised.

However, after the first year, the risk shifts, with females becoming more susceptible due to anatomical factors, including their shorter urethra, which is closer to the anus and facilitates bacterial entry. Symptoms of UTIs vary by age; infants may show non-specific signs like fever, irritability, poor feeding, or vomiting, while older children might experience painful urination, frequent urges, lower abdominal pain, and foul-smelling or cloudy urine. Fever can occur if the infection reaches the kidneys. Risk factors for UTIs include congenital urinary tract abnormalities, dysfunctional voiding, constipation, and VUR.
Diagnosis involves urinalysis, urine culture, and kidney ultrasound, with treatment typically consisting of oral antibiotics; severe cases may require hospitalization with intravenous antibiotics. Surgical correction, such as ureteric reimplantation, may be necessary for conditions like VUR and other abnormalities that cause recurrent UTIs. Preventive measures include maintaining proper hygiene, treating constipation, and circumcision in males, which has been shown to reduce UTI risk in infancy. Long-term prophylactic antibiotics and surgical procedures may be needed for recurrent UTIs, especially in children with VUR.
Tiny Fighter: Dr. Prabhu Karunakaran Helps 5-Month-Old Recover afterInnovative Stone Removal
Tiny Fighter: Dr. Prabhu Karunakaran Helps 5-Month-Old Recover afterInnovative Stone Removal
Hyderabad, April 2024 – In a remarkable display of medical innovation, Dr. Prabhu Karunakaran, a Pediatric Urologist, successfully performed a no-scalpel cystolithotripsy procedure on a 5-month-old girl, removing a bladder stone without surgical incisions. The infant, from a farmer’s family in Nakarakal Mandal, Nalgonda district, Telangana, benefitted from this minimally invasive technique that uses advanced laser technology to break down the stone into tiny particles, which are then naturally passed through urination, reducing discomfort and speeding up recovery.

The baby presented with symptoms of passing small stones during urination and frequent fever episodes. An ultrasound revealed an 8 mm stone in her bladder and mild bladder wall thickening (cystitis), while her kidneys remained normal. After careful evaluation, Dr. Karunakaran and his team decided on cystolithotripsy under general anesthesia. They employed a Thulium Fiber laser to fragment the stone into particles smaller than 2 mm, which were successfully removed without complications.
Post-surgery, the focus shifted to pain management and preventive care, with regular follow-ups scheduled to monitor the baby’s kidney function and overall health to ensure smooth recovery. “Bladder stones in infants are rare and often challenging to diagnose early,”

explained Dr. Karunakaran. “They can be caused by factors like family history, concentrated urine, or urinary tract abnormalities. This case highlights the importance of early detection and timely intervention. Our aim was to minimize discomfort and provide a safe and effective solution.” The success of this procedure underscores the importance of advanced medical technology and specialized pediatric care in managing rare conditions like bladder stones in infants. Dr. Karunakaran’s expertise and dedication to utilizing innovative solutions have proven instrumental in delivering comprehensive care for pediatric patients. For more insights, watchDr. Karunakaran’s video on YouTube: https://youtu.be/bZy5p9cyv4Y?feature=shared
Kidney Stone Symptoms in Children: How They Differ from Adults
Kidney Stones in Children A Challenge for Early Diagnosis
Author: Dr. Prabhu Karunakaran, Consultant Pediatric Urologist
A recent article published in the Times of India highlights the challenges of diagnosing kidney stones in children due to the subtlety of their symptoms compared to those typically observed in adults. Dr. Prabhu Karunakaran, a Consultant Pediatric Urologist, sheds light on the often vague and less severe symptoms that can lead to delays in treatment for young patients.
While adults commonly experience sharp pain in the lower back or abdomen when suffering from kidney stones, children may not display such obvious signs. Instead, their symptoms can be easily mistaken for other conditions, complicating early diagnosis.

Children may report mild to moderate stomach pain, which can easily be confused with other ailments. Nausea and vomiting are frequently seen in children with kidney stones and can occur without the intense pain typically associated with adults. Additionally, difficulties in urination, painful urination, and the presence of blood in the urine can also indicate kidney stones in children. Recognizing these symptoms early is crucial for effective treatment and management. Awareness among parents and caregivers is essential to ensure that children receive prompt medical attention.
Midnight Emergency: A Critical Airway Rescue
Midnight Emergency: A Critical Airway Rescue

Pediatric Lithotripsy Mastery: Safeguarding Against Complications
Pediatric Lithotripsy Mastery Safeguarding Against Complications
Delivered a talk on How to avoid complications in Pediatric lithotripsies as National faculty at PESICON held at Agra India from 8th to 10th March Dr Prabhu Karunakaran delivered a talk relevant to Pediatric lithotripsy complications- discussing how to avoid complications when treating children with kidney stones and performing the procedures safely in children. Also describing all modalities of treatments of stones in children elaborately could help colleagues to understand how to avoid complications in treating children with stones
